Hernia is far more common than most people realize with more than 5 million Americans currently living with a hernia, and surgeons performing over 1 million hernia repairs every year in the United States, alone, according to American College of Surgeons 2024 data. Despite being so common, many people ignore a hernia until it becomes painful or dangerous.
What Is a Hernia, Really?
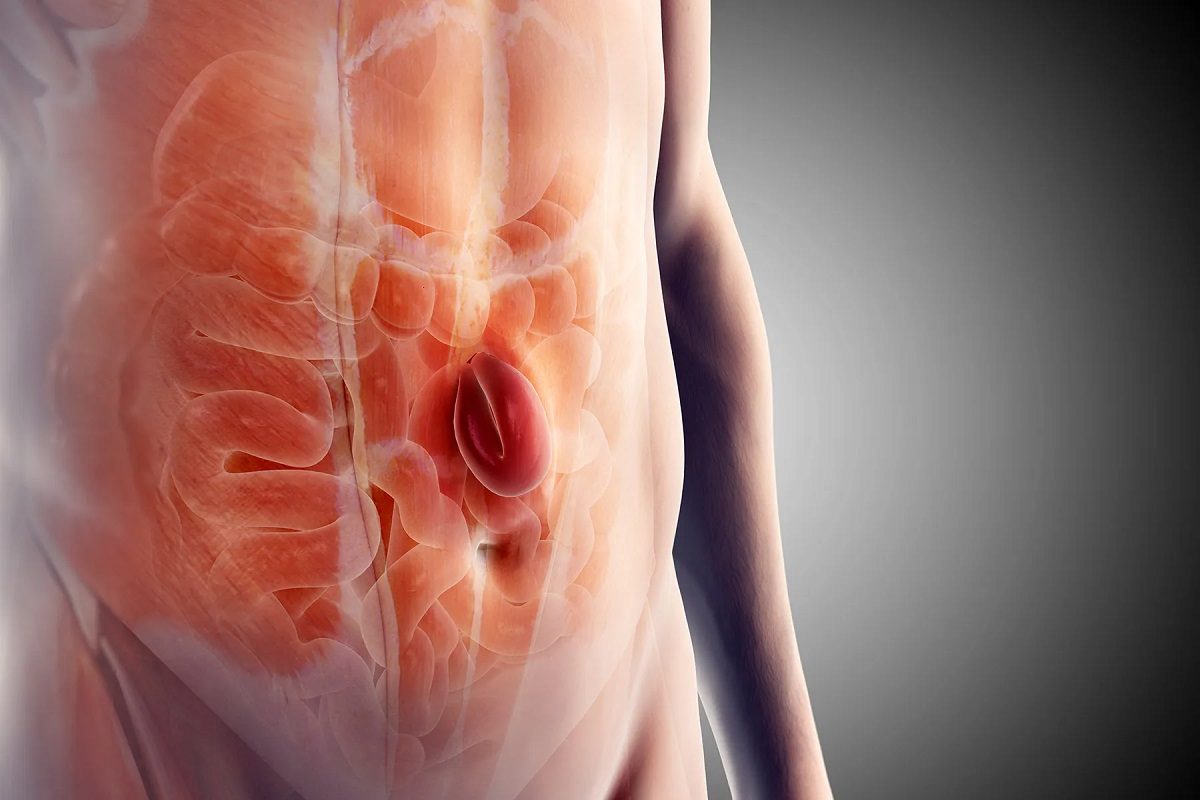
A hernia happens when an organ or fatty tissue squeezes through a weak spot in the surrounding muscle or connective tissue. Picture an inner tube bulging through a damaged tire — the “tire” is your abdominal wall, and the “inner tube” is usually intestine or abdominal fat.
Most hernias are abdominal, but they don’t heal on their own, and they almost always get worse over time. According to the Mayo Clinic: “Hernias by themselves may be asymptomatic, but nearly all have a potential risk of having their blood supply cut off (becoming strangulated). If the hernia sac contains bowel and becomes strangulated, the patient can face a life-threatening situation”.
Types of Hernia: Which One Do You Have?
There are several distinct types, each occurring in a different location and affecting different groups of people.
Inguinal hernias (groin hernias) are by far the most common, making up about 70–75 % of all hernias. They occur in the groin area and are dramatically more common in men (90 % of cases) and in baby boys. There are two subtypes: indirect (congenital) and direct (acquired later in life).
Malaria: Causes, Symptoms, Diagnosis & Effective Treatment Options
Femoral hernias appear just below the groin crease in the upper thigh. They are much less common (only 3–5 % of hernias) but disproportionately affect women and are considered the most dangerous because they have the highest risk of strangulation.
Umbilical hernias bulge at the belly button. They are very common in newborns (most close on their own by age 4–5), but also appear in adults — especially obese individuals and women after pregnancy (10–20 % of adult hernias).
Incisional or ventral hernias develop through a previous surgical scar and account for 15–20 % of cases. Anyone who has had abdominal surgery is at risk.
Hiatal hernias are different — the upper part of the stomach pushes up through the diaphragm into the chest cavity. They affect 5–10 % of the population, especially people over 50 and those who are overweight, and are the main cause of severe GERD.
Less common types include epigastric hernias (between the navel and breastbone), rare Spigelian hernias on the side of the abdominal wall, and parastomal hernias that form beside an ostomy (colostomy/ileostomy) site.
| Type | Location | Who It Affects Most | % of All Hernias | Risk of Strangulation |
| Inguinal (groin) | Groin (direct or indirect) | Men (90 %), children | 70 % | Moderate-high |
| Femoral | Upper thigh/groin (below inguinal ligament) | Women > men | 3–5 % | Very high |
| Umbilical | Around belly button | Infants, obese adults, women post-pregnancy | 10–20 % | Moderate |
| Incisional/Ventral | Through previous surgical scar | Anyone with prior abdominal surgery | 15–20 % | High |
| Hiatal | Stomach pushes through diaphragm into chest | Adults >50, obese | 5–10 % | Low (but causes GERD) |
| Epigastric | Between navel and breastbone | Adults | <5 % | Low |
| Spigelian | Side of abdominal wall (rare) | Adults | <2 % | Very high |
| Parastomal | Around stoma (ostomy patients) | Ostomy patients | 1–3 % | High |
Meningitis: Causes, Symptoms, Diagnosis & Treatment Options
Causes & Risk Factors: Why Hernias Develop
Every hernia results from the same basic equation: muscle weakness + increased abdominal pressure.
Some people are born with the weakness — for example, baby boys often have an indirect inguinal hernia because a natural tunnel (processus vaginalis) that should close before birth stays open. In adults, the weakness is usually acquired over time: chronic coughing from COPD or smoking, years of heavy lifting, chronic constipation, obesity, pregnancy, previous surgery, or simply aging collagen.
The two strongest modifiable risk factors identified in 2024–2025 research are smoking and obesity — both dramatically increase recurrence rates after repair.
Symptoms: How to Spot a Hernia Early
Most hernias start with a noticeable bulge that may come and go. The bulge typically gets bigger when you stand, cough, strain, or lift something heavy, and it often disappears when you lie down. Many people describe a dull ache, burning, or dragging sensation in the groin or abdomen, especially at the end of the day.
Hiatal hernias are an exception — they usually cause heartburn, acid reflux, chest pain, or trouble swallowing rather than a visible bulge.
Emergency “red flag” symptoms that demand immediate medical attention include sudden severe pain, a bulge that becomes hard and will not go back in, nausea, vomiting, fever, or inability to pass gas or stool. These can signal incarceration or strangulation and require same-day surgery.
Diagnosis: How Doctors Confirm It
Diagnosis almost always starts with a simple physical exam — the famous “turn your head and cough” test for groin hernias. If the exam is unclear (common in women or obese patients), doctors use ultrasound as the first imaging choice because it’s fast, cheap, and accurate. CT or MRI scans are reserved for complex, recurrent, or hidden hernias. Occasionally, diagnostic laparoscopy is performed when the diagnosis is still uncertain — the same procedure can fix the hernia at the same time.
Treatment Options for Hernia
Watchful Waiting
Small, painless inguinal hernias in men can sometimes be safely watched, but a landmark 2023 JAMA Surgery study showed that about 70 % eventually need surgery within ten years. Regular follow-up is essential.
Open Hernia Repair
The traditional operation is still widely used. Surgeons make an incision over the hernia, push the tissue back, and almost always place a lightweight mesh to reinforce the wall. It remains the go-to method when infection is present or the defect is very large.
Sickle Cell Disease: Causes, Symptoms, Diagnosis & Treatment Options
Laparoscopic (Keyhole) Repair
Using several tiny incisions and a camera, surgeons place mesh from the inside. Recovery is faster and postoperative pain is lower. It’s especially good for bilateral or recurrent hernias.
Robotic-Assisted Hernia Repair
The da Vinci robotic platform is now used in the majority of hernia repairs at high-volume centers. It offers 3D vision, wristed instruments, and tremor elimination. Robotic repair is said to have the lowest rate of chronic pain (<3 %) and allows most patients to return to work in 7–10 days.
No-Mesh (Pure Tissue) Repairs
Techniques like the Canadian Shouldice or Indian Desarda repair avoid mesh entirely. They are reserved for young patients with excellent tissue quality or those who refuse mesh.
Hiatal Hernia & Reflux Surgery
Most hiatal hernias are first treated with weight loss and acid-suppressing medication. When surgery is needed, laparoscopic fundoplication (wrapping the stomach around itself) or the newer LINX magnetic ring device can dramatically reduce reflux.
Emergency Surgery
If the hernia is strangulated, surgery must happen immediately — often with bowel resection if tissue has died.
Recovery Timeline
Patients having robotic or laparoscopic repair typically go home the same day, return to desk work in 5–10 days, and resume heavy lifting in 3–4 weeks. Traditional open repair patients usually need 2–4 weeks off desk work and 6–12 weeks before heavy lifting.
Thyroid Disorders: Symptoms, Causes, Diagnosis & Treatment Options
Prevention: Reduce Your Risk of Hernia
While you cannot change genetics, you can:
- Maintain a healthy weight
- Treat chronic cough and constipation early
- Quit smoking
- Use proper lifting mechanics
- Strengthen your core safely (avoid crunches if you already have a hernia)
Hernias never heal on their own, and the complications of waiting — strangulation, emergency surgery, possible bowel loss — are far worse than planned, elective repair. If you notice a bulge that comes and goes, groin discomfort after activity, or reflux that won’t respond to medication, see a hernia specialist, don’t wait until it becomes an emergency. Early repair is almost always the smartest, safest choice.
Syphilis: Stages, Symptoms, Diagnosis, Treatment & Prevention
