Meningitis is a medical emergency that strikes fear worldwide — and for good reason. Inflammation of the protective membranes covering the brain and spinal cord can progress from first symptoms to death in as little as 24 hours. In 2023–2024 alone, major outbreaks of meningococcal meningitis in Africa, the Middle East, and even the U.S. reminded us this disease is far from eradicated.
The World Health Organization’s 2024 roadmap aims to defeat meningitis by 2030, yet an estimated 250,000–300,000 people still die annually, and survivors often face permanent disabilities.
What Is Meningitis?
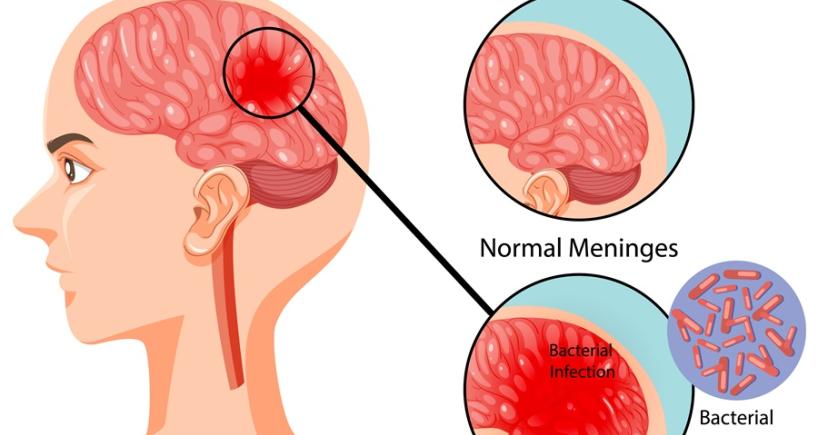
Meningitis is inflammation of the meninges — the three protective layers (dura mater, arachnoid, pia mater) and cerebrospinal fluid (CSF) surrounding the brain and cushioning the brain and spinal cord.
It is classified by cause:
| Type | Most Common Causes | Severity & Speed | Case Fatality Rate (untreated) |
| Bacterial | Neisseria meningitidis, Streptococcus pneumoniae, Haemophilus influenzae, Listeria, Group B Strep | Extremely severe, hours to days | 70–90% |
| Viral (“Aseptic”) | Enteroviruses (most common), herpes simplex, varicella, mumps, COVID-19 | Usually milder, self-limiting | <1% |
| Fungal | Cryptococcus, Candida, Histoplasma | Slow, weeks–months | 30–50% even with treatment |
| Parasitic | Naegleria fowleri (“brain-eating amoeba”) | Fulminant | >97% |
| Non-infectious | Autoimmune, cancer, drug-induced | Variable | Depends on cause |
Bacterial meningitis is the true emergency — every hour of delayed antibiotics increases mortality by ~13%.
Hernia: Types, Causes, Symptoms & Treatment Options
Causes & Transmission of Meningitis
Bacterial Meningitis
- Neisseria meningitidis (meningococcus) — lives in the nose/throat of 5–10% of healthy people (carriers). It spreads by respiratory droplets or saliva (kissing, sharing drinks).
- Streptococcus pneumoniae (pneumococcus) — most common in adults >50 and children. Often follows sinusitis, ear infection, or pneumonia.
- Haemophilus influenzae type b (Hib) — nearly eliminated in countries with Hib vaccine.
- Listeria monocytogenes — foodborne (soft cheeses, deli meats, melons); dangerous in pregnant women, newborns, elderly.
- Group B Streptococcus — leading cause in newborns.
Viral Meningitis
Usually spread fecal–oral (enteroviruses) or respiratory (mumps, measles, herpes).
Fungal & Parasitic
Immunocompromised patients (HIV, chemotherapy) or freshwater exposure (Naegleria).
Symptoms: The Red Flags You Must Never Ignore
Classic triad (present in only ~44% of adults):
- Fever
- Neck stiffness
- Altered mental status
Early symptoms (first 6–12 hours)
- High fever, severe headache
- Nausea, vomiting, photophobia (light sensitivity)
- Muscle/joint pain, extreme fatigue
Later or severe signs (12–24 hours)
- Stiff neck (positive Kernig/Brudzinski signs)
- Confusion, drowsiness, seizures
- Petechial or purpuric rash (especially meningococcal — “does not blanch” under glass test)
- Coma
Malaria: Causes, Symptoms, Diagnosis & Effective Treatment Options
In babies & toddlers
- High-pitched cry, bulging fontanelle
- Refusing feeds, irritability, limpness
- Cold hands/feet despite fever
The rash of meningococcal sepsis can look like tiny red pinpricks at first and progress to large purple bruises within hours. Therefore, seek immediate medical care if you or your child develops fever, severe headache, confusion, or stiff neck.
Diagnosis: Speed Is Everything
Diagnosis must be made within hours. Diagnosis include:
- Lumbar puncture (spinal tap) — gold standard
- CSF is cloudy in bacterial meningitis
- Key findings: low glucose, high protein, high white cells (neutrophils in bacterial, lymphocytes in viral)
- Blood cultures & PCR
- Meningococcal and pneumococcal PCR on blood/CSF gives results in <2 hours
- CT scan before LP
- Only if signs of raised intracranial pressure (papilledema, focal neurology, coma)
- Rapid antigen tests or Gram stain
- Can give preliminary results in 30–60 minutes
Sickle Cell Disease: Causes, Symptoms, Diagnosis & Treatment Options
Treatment Options for Meningitis
Meningitis treatment is mostly dependent on the causative agent:
Bacterial Meningitis (Medical Emergency)
Patient should be administered immediate empiric IV antibiotics + dexamethasone (steroid) within 1 hour of suspicion:
| Likely Pathogen | First-Line Antibiotics (2025 Guidelines) |
| Community-acquired (all ages) | Ceftriaxone 2 g IV q12h + Vancomycin (covers resistant pneumococcus) + Dexamethasone 10 mg IV q6h × 4 days |
| Age >50 or immunocompromised | Add ampicillin (for Listeria) |
| Penicillin-allergic | Substitute with chloramphenicol or meropenem |
Duration: 7–21 days depending on organism.
- Acyclovir is added if herpes encephalitis cannot be ruled out.
- Close contacts receive prophylaxis (ciprofloxacin, rifampin, or ceftriaxone).
Viral Meningitis
Supportive care only (hydration, pain relief). Most recover in 7–10 days.
Fungal Meningitis
Amphotericin B + flucytosine, then long-term fluconazole.
Parasitic (Naegleria)
Miltefosine + multiple other drugs — still almost universally fatal.
Thyroid Disorders: Symptoms, Causes, Diagnosis & Treatment Options
Long-Term Complications and Survivorship
Even with treatment, 10–20% of bacterial meningitis survivors suffer permanent damage such as:
- Hearing loss (most common)
- Seizures, cognitive deficits
- Limb amputations (from meningococcal sepsis)
- Psychological issues
Early rehabilitation and cochlear implants can help.
Meningitis remains one of the few infections that can kill a healthy person in under a day. Yet with modern vaccines, rapid diagnostics, and immediate antibiotics, survival rates have improved dramatically in high-resource settings.
Syphilis: Stages, Symptoms, Diagnosis, Treatment & Prevention
